History of manual cranial technique
Where did its elements come from, and who can be said to be the inventor? This article briefly presents historic figures in the evolution of craniosacral therapy.
Any knowledge of cranial anatomy and physiology that predates the scientific method has left no heritage of written or reliable evidence behind for modern scrutiny. The ancient Egyptian dynasties may have had more knowledge than is apparent from archeological evidence.
Millennia later in the same area, Hierophilus of Chalcedon and Erasistratus of Kios, and the Alexandrian Medical School investigated cranial function, but the information has not survived.
Anthropological folk arts such as head binding, where the growing skull of an infant is strapped with flat boards to shape its adult dimensions, demonstrate and apply an understanding of sutures and the pliability of growing cranial bones, and were preserved by cultural practices into the twentieth century.
An ancient skull from Bulgaria demonstrates that early man could crudely remove the central sphenoid bone without disturbing the other cranial bones, View photographs of this skull in a separate article Cranial mobility known in ancient times?
This procedure shows some ancient knowledge of the fact that the skull segments do not irrevocably fuse together, as is taught in modern anatomy texts.
If the sutures actually do fuse, the missing sphenoid bone could not have been removed. Do the skull bones move or not? This question has two distinct and incompatible modern answers.
A woodcut illustration from Rene Descartes’ ‘Trait de l’homme’ is presented and discussed below. This is the earliest known, if obscure, reference to the cranial rhythm and needs further research.
Sutherland’s role in cranial therapy history is re-evaluated in the light of research by David B Fuller in his 2008 paper ‘Swedenborg’s Brain and Sutherland’s Cranial Concept’.
RENE DESCARTES 1596 – 1650
The famous French philosopher and mathematician is not associated with cranial therapy history in osteopathic, craniosacral or history-of-medicine texts. The relevance of an intriguing woodcut illustration may have been overlooked. It appears in Rene Descartes’ ‘Traites de l’homme’, written in 1633 and postumously published in French in 1664.
In this interpretation of work by Rene Decartes, the top illustration represents Flexion, or the expansion phase of the cranial rhythm, with the central figure H, the pineal gland, being uprightly positioned in the hollow ventricles which have a more convex nature, possibly responding to influence M, an idea in action?.
Abundant energy is radiating, coinciding with a larger ventricular volume, where three extra A’s and an a exist, compared to the bottom illustration. Greater activity at the ventricle edges is shown and toned brain tissues B and C activate the ‘nerves’ D, which look taut.
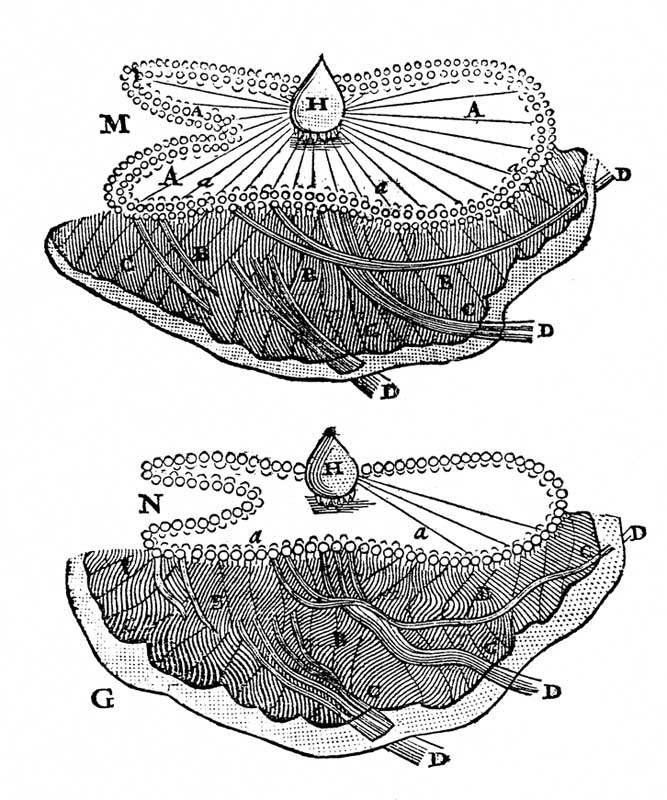
In contrast, the lower figure shows the Extension, or contraction phase of the cranial rhythm, with the pineal gland H in a less vigorous state, creating a smaller ventricular volume of concave shape, lesser edge activity, weaker brain tone at B and C (with the fissure lines between the brain lobes looking more wavy), leading to slacker ‘nerves’, possibly as a result of N a different idea or influence.
Descartes’ pre-occupation here is the pineal gland, which he saw as the physical expression of will and direction in the human organism. His physiological concepts of animal spirits and vital spirits, while couched in 17th century terms, are not wholly incompatible with a modern understanding of ion potentials in nerves.
The question of whether Rene Descartes had ever imputed or observed the existence of the cranial rhythm, that William G Sutherland would later investigate and understand in the twentieth century, is purely speculative.
This illustration alone hints at such a link. Nevertheless, the similarities between the meaning of Descartes’ illustration and Sutherland’s Primary Respiratory Mechanism (that produces the cranial rhythm) are striking and thought provoking for cranial therapists and researchers in the modern era.
https://plato.stanford.edu/entries/pineal-gland/
EMMANUEL SWEDENBORG 1688 – 1772
Emmanuel Swedenborg’s ‘The Brain’ was written from 1743 to 1744, almost 200 years before William Sutherland’s ‘The Cranial Bowl’ was published in 1939. Swedenborg was a philosopher and early brain theorist not involved with clinical practice. While he devised no techniques, his four-part scheme of brain action was used, with a fifth sacral element added, by Sutherland.
David Fuller’s paper Swedenborg’s Brain and Sutherland’s Cranial Concept provides convincing evidence that this is no mere coincidence, and examines the link between Swedenborg’s theory in the eighteenth century and Sutherland’s theory in the mid-twentieth century,
WILLIAM SUTHERLAND 1873 – 1954

While Fuller’s original and thorough article provides fresh insight into the history of cranial therapy, Sutherland’s place as the ‘father of cranial osteopathy’, originator and pre-eminent figure in this field remains unchallenged.
Sutherland was a clinician, teacher, writer and researcher whose 5-point scheme of the Primary Respiratory Mechanism (the physiology that creates the cranial rhythm) exactly mirrors the first four of Swedenborg’s scheme, plus a fifth sacral dimension added by Sutherland. Fuller demonstrates that this is no co-incidence.
Sutherland wrote one slim volume, ‘The Cranial Bowl’, in 1939. The biography ‘With Thinking Fingers’, written by his second wife, Ada Strand Sutherland, provides interesting detail on the man and his work. At the end of his career two other, more comprehensive books were published that drew on his lectures to students. ‘Teachings in the Science of Osteopathy’ and ‘Contributions of Thought’ are both classic works worthy of extended study by the committed student.
His analogy between respiratory breathing and the cranial concept, ‘The Breath of Life’, was apt for students at the time when this work was unknown. Since then the analogy has caused some confusion in those trying to understand this therapy field, as cranial motion and breathing cycle dynamics become blurred.
Sutherland considered that his work extended (into the cranial field) the philosophy and techniques of his teacher, the father of Osteopathy, Andrew Taylor Still. Since Sutherland’s time over 50 years ago, the cranial therapy field has progressed, splintered and become popular despite its scientific underpinnings remaining underdeveloped and controversial. In time, Sutherland’s legacy will inevitably be integrated into mainstream healthcare systems, after the science is better established and accepted.
NEPHI COTTAM 1883 – 1966
‘The story of Craniopathy’ was published shortly before Sutherland’s book and began the chiropractic tradition.
“Although Nephi Cottam was aware that motion of the cranial boes was palpable, his procedures relied on observation of cranial landmarks, assymetries and symptoms to provide indications for the need to manipulate particular cranial bones.” (Pederick) see Chiropractic in the cranial field
also I.N. Toftness, DC, Cranial Technique, Shell Lake, Wisconsin, 1932
Sacro-Occipital Technique as practised by chiropractors worldwide owes a debt to Major Bertrand deJarnette in developing technique and promoting its teaching and clinical use. Direct technique is frequently used in SOT, often with breath assistance, rather than the cranial rhythm, as a physiologic motor force to engage with therapeutically.
JOHN UPLEDGER 1932 – 2012
Any investigation into who originated manual cranial therapy must include Dr John Upledger and his organisations, as pioneering status claims are made and widely disseminated. A great number of practising craniosacral therapists believe he invented it. Although CranioSacral Therapy is commercially trademarked, the term itself is to be found in cranial osteopathic texts dating from at least the 1940’s. “The force behind the Craniosacral mechanism” by Dr Thomas L. Schooley, JAOA, 1948 is an example.
The following quote, and many other similar writings and advertisements, presents information that is disingenuous. “Dr Upledger trained as a surgeon and clinical researcher. His in-depth investigation into the field of cranial manipulation was prompted by an observation of a dural membrane rhythmic motion during a patient’s neck surgery in the early 1970’s. After much research Dr Upledger theorized that cranial bones continue to move into adulthood – a process previously thought to occur only in infants.”
The last line of the quotation above presents craniosacral as Upledger’s own idea, when in fact it was well-known as the fundemental assumption of Osteopathy in the Cranial Field for decades before his time. In the United States osteopathy includes medical surgery. Upledger was an osteopath who joined Sutherland Cranial Teaching Foundation classes already conducted for twenty years by the time he studied in the 1970’s, and that continue to this day.
His first text presented cranial work in an understandable way and remains seminal, combining illustrative material with anatomy, technique and research. Upledger’s role was literally as a ‘pioneering developer’ of this field, not inventor, and as a valuable commercialiser who spread the word of this important therapy from (primarily) the nurturing confines of cranial osteopathy to a much wider audience in many parts of the world.
CONCLUSION
The different professional groupings each have their own versions of history and technique. Ancient and folk elements of this field have been presented in this article to show the roots of modern cranial understanding. When competing claims for pioneering status arise, it is well to remember that knowledge is a product of its time, or as Isaac Newton put it, we are all intellectual successors standing on the shoulders of the giants that preceded us all.
The true birth of cranial therapy as a research-based, clinically-driven and anatomically relevant science of depth and breadth, incorporating numerous techniques and implications for further work, begins with William Sutherland.
Continuing the analogy, craniosacral and other members of the cranial therapy family have reached adolescence. Adulthood will occur when the transition is made from a therapy still residing within non-medical models to mainstream public healthcare systems.
Sceptics are supported by current anatomy and physiology: “Why Cranial Therapy Is silly” states that “Its underlying theory is false because the bones of the skull fuse by the end of adolescence and no research has ever demonstrated that manual manipulation can move the individual cranial bones.”
Scientific validation of key concepts such as cranial bone mobility and the existence of the cranial rhythm remains the key barrier to this development, along with sociological issues deriving from its non-medical history.