How fast or slow is the CRI? What do researchers and authors report? Is there a difference between them?
C.R.I. RATES
A critical review of the literature reporting the rate of the Cranial Rhythmic Impulse
By Malcolm Hiort Grad.Dip.Heal.Th.
Research project at Victoria University of Technology 1997
Abstract
Previous research has attempted to numerically define the normal rate of the Cranial Rhythmic Impulse (CRI). This review of the literature has identified and tabulated these studies and in doing so has deduced that the range of values given is broad if the same phenomenon, measured in the same way, is authentically described by each study cited.
Put another way, the vital question is: does an experimental study that measures a mean CRI rate of less than four cycles per minute accurately refer to the same event as that which another author contends is 14 c.p.m.?
The C.R.I. is a slow pulsatile movement phenomena, the rate of which is disputed by different authors and researchers. “The existing literature is contradictory regarding the rate of the C.R.I. …” (Myers 1997 p16)
The use of different methodologies makes meaningful comparisons difficult. Further research that includes standardised measurement as a precondition may determine an accurate and reliable reference rate for the Cranial Rhythmic Impulse.
KEY WORDS: Cranial Rhythmic Impulse, Rate of C.R.I., Primary Respiratory Mechanism, William Sutherland, Cranial Osteopathy, Craniosacral, Palpation, Measurement
1 Introduction
2 Methods
3 Results
Table 1 Reported rate of CRI
Table 2 CRI Measurement parameters
4 Discussion
-Clinical relevance
-Measurement principles
-Variability
5 Conclusion
6 Glossary
7 References / Footnotes
8 Bibliography
- 1 Introduction
The term ‘Cranial Rhythmic Impulse’ describes slow pulsatile movements that the body exhibits. This paper examines one aspect of the CRI, its rate, expressed as the number of CRI cycles per minute. The purpose of this study is not to debate the existence of the CRI, but to present and analyse all material published on this topic. What does the literature say about the rate of the CRI and upon what basis are these numeric values quoted? Is there a reliable reference rate for clinical and research purposes?
“I always thought that everyone knew that the CRI runs at about 8 to 12 cycles per minute, so when treating a brain-damaged patient with a CRI which I think is running at 3 cycles per minute, it would at least be nice to know what ‘normal’ might be.” (Vigers p12)
This quotation neatly illustrates the clinical background to this topic.
- 2 Methods – not included here
- 3 Results – Table 1 and Table 2
All known written references to the rate of the CRI up to 1996 have been tabulated for ease of comprehension in Table 1.
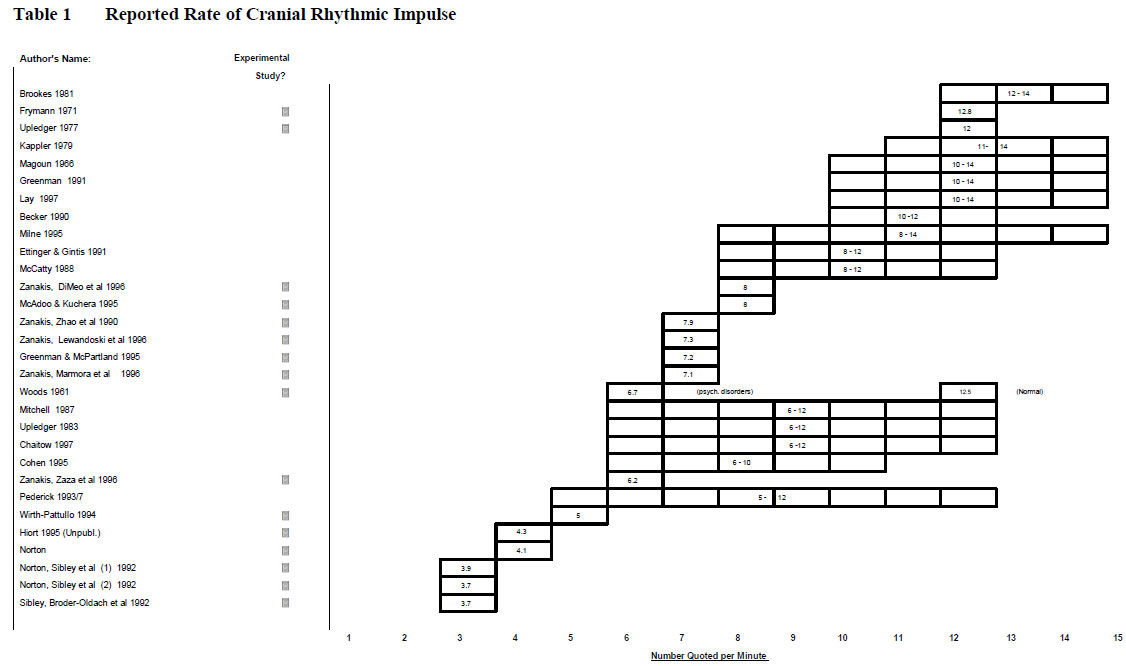
Table 1 Cranial Rhythm rate values
Where these rates are based on actual experimental studies, as opposed to an author’s opinion, various parameters have been presented for comparison in Table 2.
 .
.
Table 2 CRI measurement parameters
- 4 Discussion
“Learn to carefully scrutinize the information about the cranial field, and the cerebrospinal fluid in particular, so as to criticize scientifically. Do not base your thinking on matters that have been passed down through the ages without critical scrutiny.” (Sutherland 1990 p7)
As William Garner Sutherland is recognised as the pioneer in this field, it is fitting to begin this analysis by reflecting on the fact that in his written material Sutherland did not specify a value for the number of times per minute that the Primary Respiratory Mechanism fluctuates. (see Footnote 1)
The PRM is a term Sutherland coined to refer to anatomic and physiologic elements that combine to produce the movement of the CRI. Sutherland himself did not use the terms impulse or cycle in his writings. He used the term ‘tide’ to refer to this phenomenon of “wave movement with successive rise and fall”. (Sutherland 1939 p56)
His model consisted of five interrelated elements: the fluctuation of the cerebrospinal fluid, the function of the reciprocal tension membrane, the motility of the brain and spinal cord, the articular mobility of the cranial bones and the involuntary mobility of the sacrum between the ilia.
The term Cranial Rhythmic Impulse was coined by Dr’s John and Rachel Woods in 1961 to describe the phenomenon of movement that the interrelated elements of the PRM produced in Sutherland’s model of rhythmic whole body motion. (Ward p1129) This movement is able to be palpated, usually by the hands of a therapist. Monitoring the CRI involves the examiner sensing rhythmic changes to the tissue positions that are palpated as pulsations wax and wane.
The lack of a common recording device has limited most past CRI research to subjective empirical approaches. The CRI is therefore difficult to substantiate to the enquiring skeptic in a meaningful way, if their novice palpation skills cannot immediately detect the subtle rhythmic motion.
CRI Measurement Devices
Since 1971 various measurement devices have been invented to record the CRI objectively, without the need for a palpating examiner. Measurement systems devised to record the CRI include: Pickoffs (Frymann), Capacitance plates (St. Pierre), Force transducers (Tettambel, Retzlaff 1975 and Cope), Strain gauges (Upledger and Karni), Infrared markers (Zanakis) and Photogrammetry (Myers).
The author is aware of research efforts using light emitting diodes (see Footnote 2) and also a system to measure laser beams reflected from the cranium (see Footnote 3). None of these methods has yet gained widespread acceptance or clinical use.
At present the phenomena of the CRI is largely unknown outside of a few specialised professions. Information relevant to this phenomena comes primarily from clinically based osteopathic research and from a variety of minor sources in the biological and diagnostic sciences.
These two streams of information have historically worked in parallel, not in tandem. Specifically, a reading of the non-osteopathic research literature reveals an examination of some rhythmic and pulsatile brain phenomena, but without reference to the slow cyclical motion characteristic of the CRI concept.
The notable exception to this is a spontaneous oscillation in systemic blood pressure (at 6 to 7 times per minute) known as Traube-Hering waves. Even allowing for the wide range of CRI values identified in this study, none are great enough to approximate the comparatively fast rhythmicities identified in the many (predominantly vascular) non-osteopathic scientific studies that have researched this area.
The study by Mayhew may be an exception, where an oscillation of 0.1 Hz is identified. This value is of the order of magnitude expected for the CRI. “… the Primary Respiratory Mechanism wave would have been of the order of less than 0.5 Hz …” (Myers, 1996 p16)
The CRI is slower than than the heartbeat and normal breathing cycles. This author palpates a CRI of 4-5 cycles per minute, a slower rate than most references. (See Table 2)
A phenomenon known as a still point is a variable period of time when the pulsations of the CRI are not evident. Although the occurrence of spontaneous or induced still points thus has obvious relevance to the rate of the CRI, this relationship is not noted in the literature.
Clinical relevance
“By evaluating the CRI for its strength, rhythm, amplitude and timing, one gets the general idea of the general physical and mental state of health of the individual at that moment.”(Royder p13) This author states explicitly what others obliquely assume. It may be useful to make a distinction here between the status of the CRI and the palpatory sensations felt at particular body locations, where mobility restrictions may mask movement.
“One of the basic tenets of craniosacral therapy is that the therapist must be able to monitor the patients craniosacral rate, not only as a way of determining the treatment methods that should be used but also as a way of determining the results or the response by the patient to those treatment methods. It would therefore seem that the ability of a therapist to measure a patient’s craniosacral rate would be absolutely essential. The therapist’s need to adjust the treatment method based on the craniosacral rate would seem to call for a very high degree of reliability to measure this presumed patient characteristic.” (Echternach p917)
While this passage identifies the importance of this issue, the clinical reasons given in support of the need for reliable measurement are questionable.
Many authors have noted the great clinical relevance of the amplitude and symmetry of the CRI and have focused on
those aspects in their writings. In comparison, there is a relative lack of written material relating specifically to the rate of the CRI.
“The CRI is to the craniosacral mechanism/motion what the apical beat is to the systemic circulation. Both are a method of monitoring what is happening in the particular system.” (McCatty p17) Although this comparison is apt, other attributes of the CRI not shared by the heartbeat are unstated.
The CRI is described in the literature as being used for much more than monitoring purposes alone. “Its diagnostic possibilities have never been fully explored.” (Magoun p86) “Beyond the clinical interest of disorders such as hydrocephalus, knowledge of the rate and pathways of circulation, of the absorption and mode of origin of the fluid is needed for intelligent therapeutic measures within the central nervous system.” (Flexner p420)
“An irregular rhythm tells the therapist the treatment must be continued until the rhythm is regular.” (Manheim p195) While not specific to the rate, this quotation may illustrate an assumption that is held concerning regularity and the rate of the CRI.
“As a rule the lowest rates were found in the most disturbed patients” (Woods p993) “If there is relative mobility in the 10 to 14 cycle per minute movement of the Primary Respiratory Mechanism, symptoms are few. If it is locked to restrict this mobility, symptoms are common.” (Becker p216)
Children are reported as having faster rates than adults. Elevated CRI rates have been associated with acute maladies and with hyperkinetic children (Upledger and Vredevoogd p243)
“The fluid, which in a healthy person pulses at between 10 and 14 beats a minute, provides the nourishment and physiological environment in which your brain and nervous system can develop, live and function. Therefore, any imbalance to the craniosacral system is passed on to the rest of the body in the form of headaches, insomnia and many other dysfunctions.” (Reinhold p33)
While somewhat misconceived, this quotation from a popular magazine illustrates the issue of an accurate and reliable reference standard for the rate of the cranial rhythmic impulse.
A person reading this magazine article may erroneously conclude that their ‘slow’ CRI rate (of say 9 cycles per minute) is the cause of their sleeplessness.
“With experience in palpation and clinical knowledge of the patients history and symptoms, the rate and amplitude become an additional diagnostic indicator of his or her state of health and is helpful in determining a prognosis. The rate of CRI may be increased slightly following vigorous physical exercise, with systemic fevers or following effective osteopathic manipulative treatment of the craniosacral mechanism. The rate may be decreased with stress (mental, emotional, physical), chronic fatigue, chronic infections, mental depression and other psychiatric conditions, chronic poisoning and other debilitating conditions ” ( Lay p905 in Ward)
“The ‘normal’ CRI rate, and the significance of this, remains very much in dispute.” (Chaitow (2) p28) While the clinical relevance of the CRI rate is of interest to therapists in this field, the implications for training are also important.
Measurement principles
While a definition of the cranial rhythmic impulse exists (Ward 1995), it is clear that it is not universally adopted. Indeed, the more one investigates this concept, the less clear it becomes as to what the numerical values reported by each author actually refer to.
This author is struck by the use of the words ‘impulse’, implying a single unidirectional movement, and ‘cycle’, which denotes a repetitive pattern of movement. The obvious question to be asked is whether the same aspect of the CRI is being observed.
An interpretation of Table 1 based on this double/half logic does not untangle the issue however. The terms ‘impulse’ and ‘cycle’ would not be so apparently interchangeable if the implications of a precise research definition were more widely appreciated.
Palpation is the principal research tool used. “When observing the rate, allow one full minute and count the number of cycles (one flexion phase plus one extension phase equals one complete cycle).” (Lay p905 in Ward) The methodology described by Wirth-Pattullo is comprehensive and could be considered as a basis for the reporting of palpation methods in future research studies. “The first time the examiner called out ‘flexion’, the research assistant began timing for 1 minute and recording on an examination form each time flexion was verbalised by the examiner.” (Wirth-Pattullo p912)
This dilemma of CRI-based or clock-based recording has been resolved by use of a method in which a switch is activated
by the foot or knee, as employed by Norton, Zanakis and others. Norton claims an interactivity between the examiner of CRI-based or clock-based recording has been resolved by use of a method in which a switch is activated by the foot or knee, as employed by Norton, Zanakis and others. Norton claims an interactivity between the examiners palpation and the subjects pulsations. Would palpation using one set of fingers constitute interaction in the way Norton claims the “standard vault hold” does?
Light pressure has been identified as critical to both palpatory and mechanical measurement. “Information from cranial therapists suggested that cranial bone movements may be influenced in magnitude and direction by minute forces. This sensitivity to constraining forces…”(St. Pierre p289) Tight pickoffs interfered with measurement in the study by Frymann. The studies by Zanakis et al using reflected markers attached to the head have a research design advantage in that pressure is not an issue.
Only a few authors state the methodology that was used in any detail. Rather than this situation being a purely formal research inadequacy alone, it is possible that the differing unstated methods used do indeed affect the resultant values regarding the rate of the CRI. The practicalities of measurement of the CRI are a possible cause of variability, involving definitional, timing and pressure issues. In some cases a total of a few hundred words constitutes the study cited in this paper.
“… published accounts are best described as case studies rather than research findings.” (Myers 1997 p16)
Variability
An examination of Tables 1 and 2 in this study shows great variability in the types of study, the methods used and the results obtained. “There exists a wide range of disagreement amongst experts as to what is and what is not normal regarding rates of pulsation.” Chaitow (2) p28
To highlight the difference between minimum and maximum CRI Rate values, consider that to achieve a rate of 14 cycles per minute, the body has only two seconds of expansion, followed by two seconds of contraction to complete a single cranial rhythmic impulse two-phase cycle.
The speed of this palpatory sensation is markedly different from that which would constitute a 4 cycles per minute rate, where fully seven seconds of movement is palpated in each phase.
Table 1 shows that experimental studies have produced lower values than academic (nonexperimental) reports of the CRI rate. Older experimental studies (Woods, Frymann, Upledger) show higher rates compared to more recent experimental studies (Zanakis, Norton, etc). It is difficult to interpret this difference. The populations that were studied by each researcher varied greatly.
Table 2 shows experimental studies that include traumatic brain injury, psychiatric conditions and different traumas in the subject populations. Few studies involve enough subjects to be statistically reliable.
An assumption of regularity of CRI pulsations may be implicit in some research. “Rhythmicities between subjects varied greatly” (Zanakis, Lewandoski p497) This observation from an experimental study highlights the issue of assumptions held about the nature of the CRI before it has been comprehensively researched.
It may be the case that individual norms are relevant, so that relative rate changes, not absolute values, should be noted. Myers identified six discrete frequencies at 2.0, 3.5, 5.5, 7.5, 9.5 and 13.0 cycles per minute and noted that it “may be that the CRI is in fact a group of frequencies and the ability of the operator to focus on a rhythm may depend on their physiological state and their training.”
As a definitive explanation of the CRI is lacking, reports in the literature that do not fit orthodox descriptions based on Sutherland’s hypothesis are difficult to interpret. A broad reading relating to clinical aspects of the ‘cranial therapy’ approach shows that the CRI appears to exhibit a complex, variable, interactive nature. This may have implications in understanding the background to Norton’s work.
A detailed examination of CRI experimental studies has not been attempted at this time as the author has been unable to obtain some research reports and has relied on abstracts in several cases. This study has outlined aspects of variability in terms of the CRI itself, the results obtained (Table 1), the definition applied, the measurement principles used and the subject populations studied.
*(Since this paper was written in 1997, it was reported in the New York Times that an author cited in this paper, the lead researcher of a New York multi-researcher team studying CRI rates, was convicted of frauds in consumer injury scams involving McDonalds and Coca-Cola. Verification with Reuters was conclusive; this was the same person. See the court report at U.S.A. v Zanakis or a longer post at CRI Measurement – a selected History
- 5 Conclusion
As a comparative study specific to the rate of the CRI has not been conducted previously, (with the partial exception of Chaitow 1and 2), this literature review has sought to identify the areas in need of clarification.
There are serious problems with both validity and reliability in most CRI studies. There are other difficulties involved in CRI research that this paper has not discussed. Given these problems, it is worthwhile questioning the current value of using various CRI rates as a training aid and clinical indicator.
Researchers have urged that greater attention be paid to this area for decades. “There is an urgent need for more research in relation to cranial rhythmic impulses.” (Woods 1961, p99-103) Interdisciplinary research that combines the theoretical and palpatory focus of ‘Cranial Therapy’ with the appropriate diagnostic technology may resolve some of the problems involved with CRI study as outlined in this paper.
Objective measurement should be a priority. “The controversy surrounding palpable phenomena will exist while it cannot be objectively verified.” (Myers 1997, p16)
An objective measurement device that is simple and portable would enable fieldwork. Surveying of particular populations may allow correlative data to be recorded to determine the effects of palpation, the occurence of still points and to determine particular clinical relationships and treatment methods with greater certainty.
- 6 Glossary
Articular – Joint surfaces where bones make contact
C.R.I. – Cranial Rhythmic Impulse
CV4 – Compression of cranial ventricle four (a ‘Still Point’ technique)
Cerebrospinal Fluid – A clear fluid similar to plasma that circulates around the C.N.S.
Cranial – Relating to the cranium (head)
Frontal – A large cranial bone in the forehead region
Iatrogenesis – Problem caused by treatment
Ilia – The two single hip bones (ilium) that contact the sacrum laterally
M.R.I. – Magnetic Resonance Imaging (a diagnostic method)
Mobility – Passive movement caused by other structures
Motility – Active movement caused by the structure itself
Occiput – The cranial bone at the back of the head, where it meets the top of the neck
Osteopathy – Science of physical healing originated by A.T. Still
P.R.M. – Primary Respiratory Mechanism (see Discussion)
Palpation – Sensing kinesthetically (usually with the hands)
Parietal – Two large paired bones forming the top and sides of the cranium
Rate – The number of times an event occurs in a given time frame (CRI per minute in this field)
R.T.M. – Reciprocal Tension Membrane – Connective tissue structure inside the cranium (inner folds of the dura mater)
Sacrum – A single curved triangular bone at the base of the spine, meeting the ilia on each side
S.B.S. – Sphenobasilar Synchondrosis of the sphenoid / occiput joint in the centre of the head
Sphenoid – A single complex, multi-articulated bone behind the face, joining the occiput bone behind
Still Point – Temporary halt in the Cranial Rhythm (induced or spontaneous)
Suture – A joint between surface cranial bones
Temporal – Two paired irregular bones at the sides and base of the skull
Vomer – A single thin triangular bone in the saggital plane behind the nose and joining the sphenoid
- 7 Footnotes
1 Although a figure of 10 to 14 two-phase cycles per minute is given in Magoun (p40) with a reference (19) citing “W.G. Sutherland Unpublished lectures and writings” and by Lay (p903 in Ward), who writes “Sutherland observed this subtle rhythmic activity by palpation and determined that its normal rate is 10-14 cycles per minute.”
Chaitow also provides a figure of 12 per second (sic) that Sutherland is reputed to have determined.
2 Osteopathy Today Sept 1997;30 ( Dufrenoy N and Woledge R )
3 Rapley, B. I. Resonance Research 2/37 Ferguson St, Palmerston North, New Zealand
- 8 Bibliography
Becker R Craniosacral trauma in the adult, Ost Annals 1976;May:21325
Boyd R Biocranial therapy: an introduction, Digest Chiro Econ. 1991;March/April:223
Brookes D Lectures on cranial osteopathy, Thorsons Wellingborough 1981
Chaitow L Palpation skills, Churchill Livingstone New York 1997
Chaitow L (1) Cranial manipulation reexamined, Int J Alt Comp Med 1997;March:29-32
Chaitow L (2) Cranial dogma reassessed, Int J Alt Comp Med 1997;May:27-32
Cohen D Introduction to craniosacral therapy, North Atlantic Berkeley 1995
Cope MK, Dunlap SH Calibration of a device for the measurement of the CRI, JAOA 1983;83(1) September:132
DiGiovanna EL, Schiowitz S An osteopathic approach to diagnosis and treatment, Lippincott Philadelphia 1991
Dunbar HS, Guthrie TC, Karpell B A study of the cerebrospinal fluid pulse wave, Arch Neurol 1966;14 June:624-630
Echternach JL Letter to the editor, Phys Th 1994;74(10) 917-918
Ettinger H, Gintis B Craniosacral concepts, Ch. 25 in DiGiovanna 1991;369
Feely RA Clinical cranial osteopathy, The Cranial Academy, Meridian, 1988
Flexner LB Some problems of the origin, circulation and absorption of the cerebrospinal fluid, Quart. Rev. Biol. 1933;8:397-422
Frymann VM A study of the rhythmic motions of the living cranium, JAOA 1971;70(May):928-945
Greenman PE Principles of manual medicine, Williams and Wilkins Baltimore 1989
Greenman PE, McPartland JM Cranial findings and iatrogenesis from craniosacral manipulation in patients with traumatic brain injury, JAOA 1995;95(3) March:182-192
Greitz D Cerebrospinal fluid circulation and associated intracranial dynamicsa radiologic investigation using MR imaging and radionucleide cisternography, Acta Radiol Suppl 1993;386:123
Hiort MM Measurement of the cranial rhythm, Unpublished 1995
Jenkins CO, Campbell JK, White DN modulation resembling Traube Hering waves recorded in the human brain, Eur Neurol 1971;5:16
Kappler RE Osteopathy in the cranial field: it’s history, scientific basis and current status, Ost Physician 1979;Feb:138
Lipton JA The cranial rhythmic impulse and headaches, AAO Journal 1994;4(3)Fall:929
Lay EM Cranial field, Ch. 64 in Ward 1997;90114
Magoun HI Osteopathy in the cranial field, 3rd Ed. Journal Printing Co. Kirksville 1976
Manheim CJ, Lavett DK The self healing body, Slack Thorofare 198
Mayhew JEW, Askew S, Zheng Y et al Cerebral Vasomotion: a 0.1 Hz oscillation in reflected light imaging of neural activity, Neuroimage 1996:4(3)Dec:183-193
McCatty RR Essentials of craniosacral osteopathy, Ashgrove Bath 1988
McAdoo J, Kuchera ML Reliability of cranial rhythmic impulse palpation, JAOA 1995;95(8) August:491 PO3
Milne H The heart of listening, North Atlantic Berkeley 1995
Mitchell F Clinical significance of cranial suture mobility, in Retzlaff 1987;13-26
Myers RG A review of the literature with respect to osteopathy in the cranial field, Aust J Ost 1996;8(2):13-19
Myers RG A review of the literature with respect to osteopathy in the cranial field, Aust J Ost 1997;9(1):14-17
Myers RG Measurement of small rhythmic motions around the human cranium in vivo, Aust J Ost 1988: 9(2): 6-13
Norton JM A tissue pressure model for palpatory perception of the cranial rhythmic impulse, JAOA 1991;91(10)October:975-994
Norton JM Failure of a tissue pressure model to predict cranial rhythmic impulse frequency, JAOA 1992;92(10) October:1285 PO8
Norton JM, Sibley G, Broder-Oldach R (1) Quantification of the cranial rhythmic impulse in human subjects, JAOA 1992;92(10) October:1285 PO7
Norton JM, Sibley G, Broder-Oldach R (2) Characterisation of the cranial rhythmic impulse in healthy human adults, AAO Journal 1992;2(3):9-26
Norton JM, Sibley G, Broder-Oldach R Documentation of the cranial rhythmic impulse, 1997
Pederick FO Cranial adjusting – an overview, Chiro. J. Aust 1993;23(3) September:10611
Pederick FO A Kaminski-type evaluation of cranial adjusting, Chiro. Tech. 1997;9(1):115
Reinhold L Craniosacral balancing, Womans Day 1997:September1:33 (Australian magazine)
Retzlaff EW, Michael DK, Roppel RM, Cranial bone mobility, JAOA 1975;74(May):869-872
Retzlaff EW The cranium and its sutures, SpringerVerlag Berlin 1987
Royder JO Fluid hydraulics in human physiology, AAO Journal 1997;7(2):116
Sibley G, BroderOldach R, Norton JM Interexaminer agreement in the characterisation of the cranial rhythmic impulse, JAOA 1992;92(10) October:1285 PO9
St. Pierre N, Roppel R, Retzlaff E The detection of relative movements of cranial bones, JAOA 1976;76(December):289
Stylian G Is craniosacral therapy cranial osteopathy? Aust J Ost 1996;8(1):145
Sutherland WG The cranial bowl, Free Press Mankato 1939
Sutherland WG Teachings in the science of osteopathy, Rudra Portland 1990
Sutherland WG Contributions of thought, 2nd Ed. Rudra Portland 1998
Tettambel M, Cicora RA, Lay EM Recording of the cranial rhythmic impulse, JAOA 1978;149
Upledger JE The reproducibility of craniosacral examination findings: A statistical analysis, JAOA 1977;76(August):890-899
Upledger JE, Karni Z Mechanoelectric patterns during craniosacral osteopathic diagnosis and treatment, JAOA 1979;78(July):782-791
Upledger JE, Vredevoogd JD Craniosacral therapy, Eastland Seattle 1983
Upledger JE Letter to the editor, Phys Th 1995;75(4)April:328
Urayama K Origin of lumbar CSF pulse wave, Spine 1994;19(4):4415
Vigers P Letter to the editor, Osteopathy Today 1997;May:12
Ward RC(ed.) Foundations for osteopathic medicine, Williams and Wilkins Baltimore 1997
Warwick R, Williams PL Gray’s anatomy, 35th Ed. Longman Edinburgh 1973
WirthPattullo V, Hayes KW Interrater reliability and craniosacral rate measurement and the relationship with subjects, Phys Th 1994;74(10)October:90816
Woods JM, Woods RH A physical finding related to psychiatric disorders, JAOA 1961;(60)August:98893
Zanakis MF, Lewandoski MA, Marmoura M, Kircher KT, Banihashem M, Dowling DJ Cranial mobility in man: objective measurements in normal subjects, JAOA 1995;95(8)August:497 016
Zanakis MF, Marmoura M, Banihashem M, Kircher KT, Lewandoski MA, FerrisPhillips MT Subjective and objective evaluations of the cranial rhythmic impulse in man, JAOA 1995;95(8)August:497 017
Zanakis MF, Kircher KT, Lewandoski MA, Schwartz D, Sussman M Accuracy of acupuncture needle markers and surface markers for obtaining the “cranial kinetogram” in humans, JAOA 1995;95(9)September:547 26
Zanakis MF, DiMeo J, Madonna S, Morgan M, Drasby E Objective measurement of the CRI with manipulation and palpation of the sacrum, JAOA 1996;96(9)September:551
Zanakis MF, Marmoura M, Morgan M, Lewandoski MA Application of the CV4 technique during objective measurement of the CRI, JAOA 1996;96(9)September:552 PO3
Zanakis MF, Morgan M, Storch I, et al Detailed study of cranial bone motion in man, JAOA 1996;96(9)September:552 PO6
Zanakis MF, Zaza W, Zhao H, Morgan R, Schatzer M Objective measurement of the cranial rhythmic impulse in children, JAOA 1996;96(9)September;552 PO5
Zanakis MF, Zhao H, Schatzer M, et al Studies of the cranial rhythmic impulse in man using a tilt table, JAOA 1996;96(9)September:552 PO4
Malcolm Hiort 1997